

Abstract
Introduction
MYC-rearrangement (MYC-R) occurs in approximately 10-15% of diffuse large B-cell lymphomas (DLBCL) and several studies suggest an inferior progression free (PFS) as well as overall survival (OS) compared to DLBCL without MYC-R. However, the prognostic significance of MYC single-hit (MYC-SH), MYC double/triple-hit (MYC and BCL2 and/or BCL6 translocation; MYC-DH/TH) in the context of the MYC translocation partner (MYC-IG versus MYC-non-IG) is less clear due to relatively small sample sizes in prior studies. The Lunenburg Lymphoma Biomarker Consortium (LLBC) set out to address these questions in a large number of DLBCL treated uniformly with rituximab (R)-CHOP- or R-CHOP-like chemotherapy.
Methods
Relevant clinical data (IPI factors, PFS, OS) from patients with aggressive B-cell lymphomas with confirmed DLBCL morphology derived from registry cohorts (Canada: British Columbia Cancer, UK: Leeds/HMRN, Barts, USA: Stanford) and prospective clinical trials (Germany: RICOVER, MegaCHOEP, France: LNH01-5B and LNH03-B, HOVON: HO 46 and 84) were pooled in the LLBC database (n=5118). Interphase FISH analysis (mostly on tissue microarrays) was used to determine the MYC-, BCL2- and BCL6-rearrangement status. All DLBCL with available tissue underwent break-apart testing for MYC (Vysis, LSI, Abbott). Identified MYC-R cases were subjected to FISH break-apart testing for the BCL2- and BCL6 loci as well as to MYC/IGH fusion testing and, if negative, to MYC/IGK and MYC/IGL testing to allow designation of the final MYC-R status (MYC-IG versus MYC-non-IG). Information on the cell of origin (COO) was generated using immunohistochemistry (Hans classifier) and/or gene expression based methods. Survival probabilities were estimated using the Kaplan Meier method and survival curves were compared with the log-rank test. The effects of variables of interest were estimated using univariate and multivariate Cox models stratified on the variable 'cohort' and 'trial'.
Results
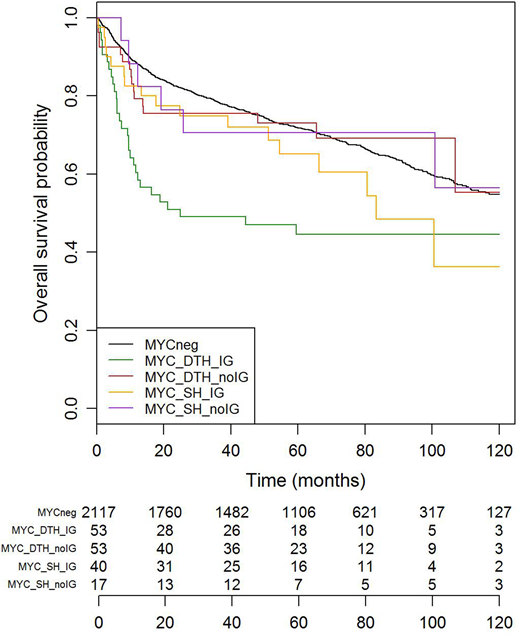
2380 DLBCL patients with full data on PFS, OS, IPI factors and MYC FISH results were available for analysis. 263 DLBCL cases (11%) had MYC-R which was associated with inferior PFS and OS compared to DLBCL patients without MYC-R (59% versus 72% OS at five years; log-rank <0.001; 56% versus 64% PFS at five years; log-rank <0.002). This effect was observed in both COO subgroups (GCB and non GCB). Out of 163 MYC-R patients with complete FISH data, 40 were MYC-SH with an IG partner (24.5%) and 17 (10.5%) with a non-IG partner. 53 patients had a MYC DH/TH constellation with an IG partner (32.5%) and 53 patients (32.5%) with a non-IG partner. The MYC-DH/TH group with an IG partner had the worst OS at 24 months: (50.9% compared to 76.4% for the remaining MYC-R DLBCL patients and to 82.4% for patients without MYC-R) (fig1). Similar results were obtained for PFS. In the MYC-DH group, there were no differences in OS and PFS between MYC/BCL2 and MYC/BCL6 'double hits'. Multivariate Cox models adjusting for the IPI and including a time-dependent effect showed, that the impact on outcomes was mainly seen in the first 24 months post therapy (hazard ratio (HR) of 2 [1.59-2.53] for MYC-R DLBCL patients compared to patients without MYC-R and a HR of 3.12 [2.09-4.64] for MYC-DH/TH tumors in which MYC is translocated to IG). In contrast, in MYC-R patients including MYC-SH and MYC-DH/TH without an IG partner, the HR was lower at 1.5 [1.01-2.24].
Conclusion
This study by the LLBC in a very large cohort of DLBCL patients treated with R-CHOP or R-CHOP-like therapy confirms previous reports on the negative prognostic impact of an underlying MYC-translocation for both PFS and OS. This impact is predominantly observed in the first two years post therapy. Further, the large sample size extends previous observations that the partner gene of MYC (IG versus non-IG) also has prognostic impact. MYC-DH/TH DLBCL with an IG partner gene have the worst OS and PFS, while impact is moderate in other constellations (MYC-SH and MYC-DH/TH with a non-IG partner). Additionally, no differences between MYC/BCL2 and MYC/BCL6 'double hits' are seen in PFS and OS. Our results suggest that along with MYC testing in routine clinical practice, identification of the MYC partner gene (IG versus non-IG) is also warranted to identify further DLBCL subsets with poor outcomes which may have implications in the design and interpretation of future clinical trials.
Sehn:Merck: Consultancy, Honoraria; TG Therapeutics: Consultancy, Honoraria; Roche/Genentech: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Morphosys: Consultancy, Honoraria; Karyopharm: Consultancy, Honoraria; Lundbeck: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal